
The condition:
The large bowel (intestine) is made up of the
colon and rectum (back passage). This part of
the digestive tract carries the remains of digested
food from the small bowel and gets rid of it as
waste through the opening to the back passage
(anus). Cells that line the colon and rectum may
begin to grow out of control, forming a tumour (a
growth of cancer cells).
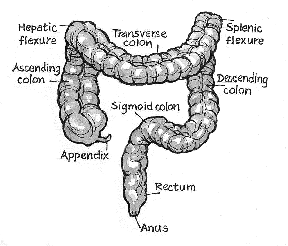
The bowel has four sections: the ascending
colon, the transverse colon, the descending colon
and the sigmoid colon. Tumours can start in any
of these areas or in the back passage. Tumours
start in the innermost layer and can grow through
some or all of the other layers.
The procedure:
Removal of the lower part of the large bowel, the
rectum (back passage) and the anal region through
the abdomen and the perineum (the skin between
the anus and the genitals). The anal area is stitched
together and will remain permanently closed. The
end of the large bowel is brought out through the
wall of the abdomen as a colostomy. This is
permanent and allows the bowel content to drain into
a bag worn over the colostomy. When the operation
is completed, the abdominal wound is closed with
stitches and/ or staples.
RISKS OF THIS PROCEDURE
There are some risks/ complications. Please read
the patient information sheet – “Major Bowel Surgery
for Tumour” for detailed information about the risks
involved.
The risks include:
(a) Leakage where the bowel was stitched to gether.
This may need further surgery.
(b) Deep bleeding in the abdomen.This may need
fluid replacement or further surgery.
(c) Bowel is paralysed, causing abdominal bloating
and vomiting. This is usually temporary.
(d) The wound may become infected. This is usually
treated with antibiotics or the wound may need
to be opened.
(e) Urinary tract infection. Antibiotics may be used
to control the infection.
(f) Infection in the abdominal cavity. This may form
an abscess that may need drainage and
antibiotics.
(g) The bowel may be u nable to be joined and may
be brought to the surface as a stoma, with the
following problems:
- The blood supply to the stoma may fail and
cause damage. This may need further
surgery. - Excess fluid loss from the stoma
- Stoma prolapse – the bowel protrudes past
the skin. - Parastomal hernia – the bowel pushes
through a weak point in the muscle wall,
causing pain - Local skin irritation – reddening of the skin
and a rash in reaction to the stoma bag glue
(h) Bleeding into the abdomen. A blood transfusion
and further surgery may be necessary.
(i) Damage to the tube bringing the urine from the
kidney to the bladder.
(j) Abnormal emptying of the bladder. It may empty
without control or may not empty at all.
(k) Inability to have and/ or maintain an erection in
men. In women, it can cause pain during or after
intercourse.
(l) The wound may be abnormal and the wound
can be thickened, red and painful.
(m) The bowel actions may be much looser after the
operation than before
(n) Adhesions (bands of scar tissue) develop in the
abdominal cavity and the bowel may block
(o) Death within 30 days of surgery is estimated at 1
in 16 to 1 in 63.