
Procedure:
This means permanently stoping the flow of sperm from the testicles to the outside, thus preventing a man from fathering children. The operation may occasionally also be used to prevent urine from refluxing along the vas (and may be used to treat recurrent infection of the tubules near and inside the testicle when non-surgical options have failed.)
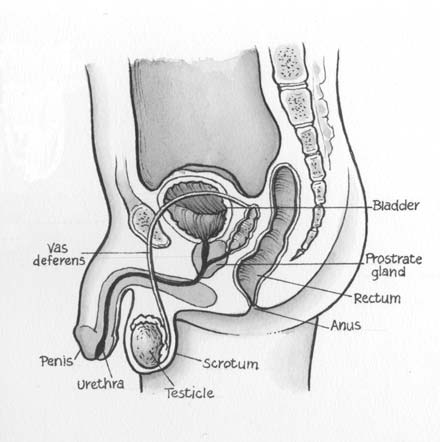
The scrotum may be shaved before being cleansed with antiseptic. Under local anaesthetic, the tube draining sperm from the testis (vas deferens) is located on each side and a small cut made in the scrotum so the vas can be seen. Several ways can be used to interrupt the vas, including removing a length. The lining of the tubes may be destroyed for a short distance to seal them, or other tissues may be placed between the cut ends of the tubes. Both sides are treated in the same way.
The choice of procedure depends on the surgeon. Any bleeding is stopped and the separated ends of the cut tubes are replaced in the scrotum. The skin may be closed with fine absorbable stiches if necessary.
Risks of this procedure:
These include:
(a) During the operation, a few men may notice a slowed heart beat and may feel faint.
(b) After the operation, you may develop a bruise in the scrotum that may take up to several weeks to resolve.
(c) You may develop an infection in the skin wound that may need antibiotic treatment.
(d) You and your partner will need to use alternative contraceptive methods for at least several weeks until ejaculate samples have been tested and you have been told they are clear of sperm.
(e) There is a very small chance ejaculates will never clear of sperm due to a technical failure. This will require a repeat operation.
(f) There is a remote chance the vas may rejoin spontaneously, even after you have been sterile for some time (re-canalisation). If this happens, you may no longer be sterile. Despite this, the operation should be regarded as permanent. Reversals can be done, but they are expensive and are not always successful. They are not available under Medicare.
(g) Sometimes a generally painful and swollen area at the back of a testicle may develop and this may persist for some months. This can be treated with scrotal support, ice packs and anti-inflammatory tablets.
(h) Small cysts may sometimes develop at the back of the testicle.
(i) Occasionally small inflammatory nodules around the cut ends of the vas or in the epididymis occur. These are unlikely to cause symptoms, but uncommonly result in some tenderness or pain with ejaculation. Most respond to simple treatments if necessary.
(j) There is a small risk of long term aching in the testicles. This is usually mild and responds to anti-inflammatory medication. In a few men, this can be persistent.
(k) Rarely, a connection may form between a cut vas and the skin. This requires surgical treatment.
(l) Increased risk in obese people of wound infection, chest infection, heart and lung complications, and thrombosis.
(m) Increased risk in smokers of wound and chest infections, heart and lung complications and thrombosis